Ever wonder why a simple ache in the heel can linger for weeks? The answer often lies in two often‑mixed‑up conditions: tendonitis is a inflammation of a tendon caused by overuse, strain, or micro‑tears and Plantar Fasciitis is a painful inflammation of the thick band of tissue (the plantar fascia) that runs along the bottom of the foot. Both can trigger stubborn heel pain, but they do it in slightly different ways. Understanding how they interact helps you pick the right relief strategy instead of spinning your wheels with generic rest and ice.
Key Takeaways
- Tendonitis and plantar fasciitis often coexist because they share risk factors like over‑pronation and tight calf muscles.
- Location of pain distinguishes the two: tendonitis hurts the tendon insertion, while plantar fasciitis hurts the arch’s heel‑side.
- Accurate diagnosis usually needs a physical exam plus imaging such as ultrasound or MRI.
- Effective treatment blends rest, targeted stretching, supportive orthotics, and guided physical therapy.
- Preventing recurrence means fixing foot biomechanics and gradually increasing activity load.
What Exactly Is Tendonitis?
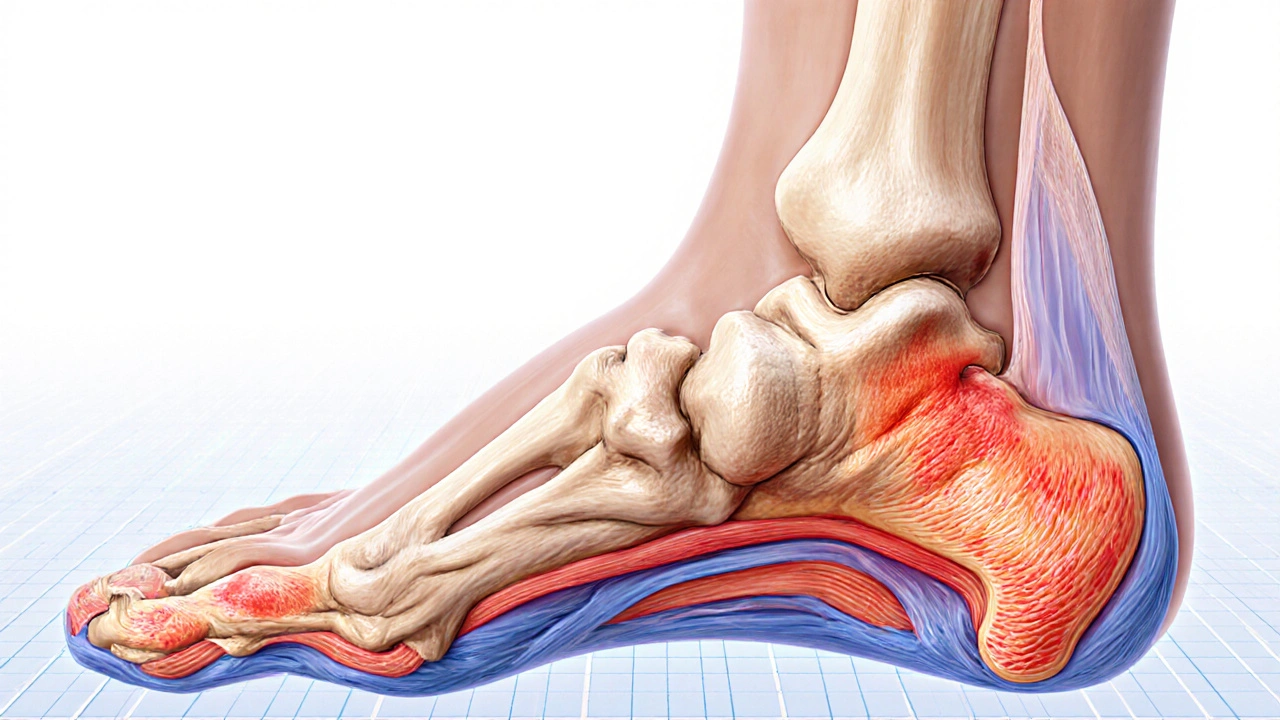
When a tendon- the tough cord that connects muscle to bone-gets overloaded, microscopic fibers tear. The body sends inflammatory cells to repair the damage, causing swelling, warmth, and pain. In the foot, the most common culprit is the Achilles tendon, which attaches calf muscles to the calcaneus (the heel bone). If the tendon swells near its insertion, you’ll feel pain high on the heel that worsens after sitting or overnight.
How Tendonitis Connects to Plantar Fasciitis
Both conditions thrive on the same set of biomechanical stresses. Over‑pronation, where the foot rolls inward excessively, stretches the plantar fascia and puts extra strain on the Achilles tendon. Tight calf muscles pull the heel upward, increasing the tension on the attachment point of both the fascia and the tendon. In short, a tight calf muscle can be the common denominator that fuels both tendonitis and plantar fasciitis.
Spotting the Differences: Symptoms and Pain Patterns
Because the conditions share origins, the pain can feel similar, but there are tell‑tale signs:
- Location: Tendonitis pain centers on the tendon’s insertion-often the back or lower side of the heel. Plantar fasciitis pain is sharpest at the front of the heel, right where the fascia meets the calcaneus.
- Timing: Tendonitis may worsen after prolonged standing or activity, while plantar fasciitis typically peaks first steps out of bed and eases after a few minutes of walking.
- Texture: Swelling or a palpable knot is common with tendonitis; plantar fasciitis usually presents a tender band along the arch.
Getting the Right Diagnosis
A healthcare professional starts with a focused foot exam-checking gait, ankle range of motion, and heel tenderness. If the picture isn’t clear, imaging helps:
- Ultrasound can reveal thickened tendons or fluid buildup.
- MRI offers a detailed view of soft‑tissue inflammation and rules out bone stress fractures.
Knowing which structure is inflamed directs the treatment plan, preventing a one‑size‑fits‑all approach that often fails.
Treatment Toolbox: From Rest to Rehab
Even though rest sounds simple, it’s only the first step. Here’s a practical roadmap:
- Load Management: Cut activities that aggravate the heel for 48‑72hours. Replace running with low‑impact options like swimming.
- Targeted Stretching: Perform calf‑gastrocnemius and soleus stretches twice daily. A common routine: stand facing a wall, place the affected foot back, keep the heel flat, and lean forward for 30seconds. Repeat three times.
- Footwear Upgrade: Shoes with good arch support and a cushioned heel reduce strain on both the fascia and the tendon.
- Orthotics: Custom or over‑the‑counter orthotics help correct over‑pronation, distributing pressure more evenly across the foot.
- Physical Therapy: A therapist can guide eccentric loading exercises for the Achilles tendon-slowly lowering the heel below a step edge-to promote tendon remodeling.
- Inflammation Control: Short courses of NSAIDs (ibuprofen or naproxen) can curb swelling, but they’re not a long‑term fix.
- Modalities: Ice packs for 15 minutes after activity, or occasional ultrasound therapy in the clinic, can accelerate healing.
Comparison: Tendonitis vs. Plantar Fasciitis
| Aspect | Tendonitis | Plantar Fasciitis |
|---|---|---|
| Primary tissue | Achilles or other foot tendon | Plantar fascia |
| Typical pain spot | Back/side of heel, near tendon insertion | Front of heel, where fascia meets calcaneus |
| Morning stiffness | Less common | Very common, sharp first steps |
| Risk factors | Over‑use, tight calf, sudden increase in activity | Over‑pronation, tight calf, improper footwear |
| Primary rehab focus | Eccentric tendon loading, calf stretching | Foot arch support, fascia stretching, night splints |
Preventing Recurrence
Once you’re symptom‑free, the goal shifts to keeping the heel happy:
- Gradually increase mileage by no more than 10% per week.
- Maintain daily calf and plantar fascia stretches-even on rest days.
- Rotate shoes; avoid wearing the same pair for more than 500km.
- Consider a periodic check‑in with a physiotherapist to tweak your gait.
When to Seek Professional Help
If pain persists beyond three weeks despite home care, or if you notice swelling, bruising, or loss of ankle strength, it’s time to see a clinician. Persistent inflammation can lead to tendon degeneration or chronic plantar fascia thickening, which may require more intensive interventions like corticosteroid injections or, rarely, surgery.
Frequently Asked Questions
Can tendonitis cause plantar fasciitis?
Yes. Tight calf muscles from Achilles tendonitis increase strain on the plantar fascia, making it easier for fasciitis to develop.
Is heel pain always plantar fasciitis?
No. Heel pain can stem from Achilles tendonitis, heel spurs, bursitis, or even stress fractures. A proper exam distinguishes the cause.
What’s the best stretch for both conditions?
A standing calf stretch against a wall targets the gastrocnemius and soleus, easing tension on the Achilles tendon and indirectly reducing pull on the plantar fascia.
Can I still run with tendonitis?
Only after the acute inflammation subsides and you’ve built up tendon strength with eccentric exercises. Jumping back in too soon often worsens the injury.
Are over‑the‑counter orthotics enough?
For mild over‑pronation, yes. Severe biomechanical issues may need a custom‑made orthotic, which a podiatrist can prescribe.
Lindy Swanson
October 1, 2025 AT 22:31Wow, another post telling us to just stretch and buy orthotics. While the basics are solid, the real issue is how most people ignore the role of progressive loading. You can’t just slap on a heel cup and expect the Achilles to heal overnight. The tissue needs a graduated stress protocol, otherwise you’re just masking the inflammation. Also, the article forgets to mention that tight calves can be a symptom, not just a cause. If you keep pulling the same muscle every day, you’re feeding the fire. A lot of the advice sounds like a one‑size‑fits‑all generic plan. Personal biomechanics matter more than a generic shoe. I’ve seen runners who follow the exact routine here and end up worse off. So, take the info with a pinch of salt and tailor it. And don’t forget to check your gait with a professional before you commit to a pricey orthotic. Bottom line: don’t treat tendonitis and plantar fasciitis as identical.
Amit Kumar
October 16, 2025 AT 20:07Great rundown of tendon and fascia issues! 😊 It’s awesome how you broke down the differences-makes it less confusing for beginners. The part about tight calves being a common denominator is spot on; I’ve felt that pull every morning before a run. I’ve been using the calf‑gastrocnemius stretch you mentioned and it’s helped reduce the ache after a few weeks. 🏃♂️ Adding a simple eccentric heel‑drop routine three times a week really speeds up Achilles tendon recovery. 👍 Also, switching to shoes with proper arch support has made my daily walks pain‑free. 🦶 Don’t underestimate the power of a good night splint; it keeps the fascia gently stretched while you sleep. 😴 Consistency is key-jumping back into mileage too soon can set you back. 🎯 I love that you emphasized gradual load increase; the 10% rule is a lifesaver for avoiding overuse. 📈 When I first started, I ignored imaging and stuck with rest, but the pain lingered until I got an ultrasound. 📹 That clarified it was tendon inflammation, not a stress fracture. 🎥 If you’re ever unsure, a quick scan can save weeks of trial‑and‑error. 🩺 Remember, inflammation control with NSAIDs is fine short‑term, but don’t rely on meds alone. 🩹 Finally, keep up the awesome detailed guides-your community benefits from clear, actionable advice! 🙌
Crystal Heim
October 31, 2025 AT 16:43Tendonitis and plantar fasciitis are distinct conditions. The inflammation location defines the pain. Achilles issues hurt the back of the heel. Fascia problems sting at the front. Over‑pronation stresses both structures. Tight calves amplify the load. Proper diagnosis avoids wasted therapy. Imaging clarifies the inflamed tissue. Stretching alone rarely solves everything. Orthotics help correct alignment. Eccentric loading rebuilds tendon fibers. Night splints relieve morning stiffness.
Sruthi V Nair
November 15, 2025 AT 14:19The foot is a marvel of biomechanics and every imbalance can echo through it. A tight calf is not just a symptom but a messenger of deeper misalignment. When you lengthen the gastrocnemius you also free the plantar fascia from excessive tension. Think of the body as a chain; pull one link and the others react. Regular mindful stretching can become a daily meditation for the lower limb. Simple wall‑calf stretches performed twice a day can shift the whole system. Consistency beats intensity when building long‑term resilience. The key is to listen to the subtle cues before pain overtakes. This perspective transforms rehab from a chore into a practice of self‑awareness.
Mustapha Mustapha
November 30, 2025 AT 11:55Thanks for sharing this comprehensive guide. It’s clear that both tendonitis and plantar fasciitis require a balanced approach of rest and targeted rehab. I’d add that monitoring load progression is essential to prevent setbacks. Gradual mileage increases and regular gait assessments can keep the healing process on track. Also, encouraging patients to rotate shoes helps distribute stress more evenly across foot structures. Keep up the inclusive tone; it makes the information accessible.
Ben Muncie
December 15, 2025 AT 09:31Ideally you’d treat the root cause, not just slap on ice.
kevin tarp
December 30, 2025 AT 07:07The article is well‑written, but there are a few grammatical slips worth noting. For example, "tendon‑insertion" should be hyphenated consistently, and "over‑pronation" needs a hyphen to match the style elsewhere. Also, avoid the split infinitive in "to properly stretch"; instead, say "to stretch properly". Maintaining uniform punctuation improves readability. Overall, great content with minor copy edits.
ravi kumar
January 14, 2026 AT 04:43While the medical advice is solid, it’s strange to see such a Western‑centric view without acknowledging traditional practices. In India we have long used Ayurvedic oil massages to improve circulation in the foot, which can complement modern stretches. Also, national health systems should promote community awareness rather than relying solely on expensive imaging. The emphasis on orthotics is good, but local craftsmen can produce effective supports at a fraction of the cost. Remember, health solutions should be adaptable to diverse economic realities.
SandraAnn Clark
January 29, 2026 AT 02:19This stuff is useful. I get that heel pain isn’t fun. Trying the stretches might help.
Rex Wang
February 12, 2026 AT 23:55Wow, this article really dives deep, and, you know, it’s packed with practical steps, and, I love how it mixes science with everyday advice, and, the pacing is just right, and, the use of bullet points makes it easy to follow, and, overall it feels like a friendly chat rather than a lecture, and, definitely worth a read.
mark Lapardin
February 27, 2026 AT 21:31The discourse surrounding musculoskeletal injuries often suffers from a lexical deficit, wherein layperson vernacular eclipses precise biomechanical terminology. This piece admirably bridges that gap by integrating rigorous pathophysiological descriptors with actionable rehabilitation protocols, thereby facilitating translational application. However, the omission of kinetic chain considerations-particularly hip internal rotation deficits-represents a missed opportunity for holistic intervention. Incorporating proximal stabilization exercises could potentiate distal outcomes, aligning with current evidence-based paradigms. Nonetheless, the synthesis of imaging modalities and functional therapy herein exemplifies a commendable multimodal framework.